
The details are still being debated, but the following are 2 well-known facts about the physician reimbursement models of the future:
- They will be based on a metric that considers quality, value, and outcomes
- The data used to stratify patients in the future will be based on the diagnosis codes that are reported now.
If we learned anything from the Physician Quality Reporting System, we know that there is an approximate 2-year gap between gathering data and using the data to impact physician penalties. Simply put, the diagnosis codes submitted on medical claims in 2016 will have a direct impact on reimbursement in 2018.
Matching ICD-10 Codes to the New Reimbursement System
The Centers for Medicare & Medicaid Services and the payer group America’s Health Insurance Plans announced in mid-February that they reached a consensus on how to measure physician quality in 7 clinical areas, from primary care to the treatment of patients with cancer or AIDS. According to a Washington Post article, the ratings “will not be used immediately,” but are intended to act as “building blocks” as private health plans and Medicare shift to value-based care.1 Medicare Advantage currently has a list of diagnosis codes that define patients who are at increased risk. “Value-based care,” “value,” “quality,” and “outcome” are words that are entirely dependent on the status of the patient at the point of care.
The International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) has impacted charge capture in many ways. Many practices are adapting well to the new levels of detail and documentation requirements within the medical record.
Social histories now consistently capture the patient’s smoking history: the impression (summarizing the patient’s situation) includes chronic conditions that impact decision-making, and all records that note metastatic disease document the primary tumor sites when they are known, which is half the battle. The second half of the battle is: each relevant detail must be translated into codes, and must be submitted on the claim form, for data mining to work effectively.
Are you coding patient encounters today to accurately reflect the whole story, or do you still report only the primary reason that the patient is seen in your practice?
It is not only about your Medicare beneficiaries. Headlines routinely highlight the significant shift in reimbursement to physicians across all payers. In March, Highmark announced that it will introduce a bundled-payment initiative that is aimed at paying for value in cancer care.2
Highmark’s new bundled-payment option includes 19 cancer types that are treated with drug therapies, as well as radiation treatment for patients with breast cancer. Instead of requiring physicians to obtain prior authorization for care, Highmark will pay them a lump sum that it will negotiate individually with each provider based on past payments the physician had received.2
Negotiating payments individually based on past payments may or may not accurately reflect the severity of your patients’ conditions or the extensive care that your patients receive. Without the data, you cannot navigate those conversations successfully.
Data-Based Reimbursement
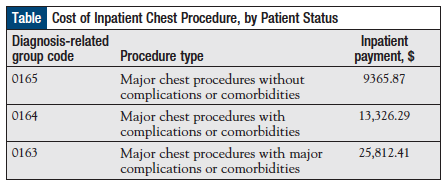
Let’s look at a very simple, straightforward example of a reimbursement system that is already in place and is anchored in the severity of the patient’s disease. Diagnosis-related groups (DRGs) are part of the inpatient prospective payment system. Patients are categorized based on the DRG, and the reimbursement is then based on the average resources that are used to treat Medicare beneficiaries in that DRG. For example, the exact same “major chest procedure” may be reimbursed to the facility at $9000 or at $25,000 (Table), depending on the status of the patient.
In this example, the procedure itself did not change, but the severity of the patient did. Health information management coders have long honed their skills at scouring charts to confirm the “complications” or “major complications” that are documented in the medical record. The only way to communicate to a payer that a patient has complications or comorbidities is through diagnosis codes.
- Does the typical “impression” on the average progress note in your practice contain the data to support the differences in severity between patients with lung cancer?
- Does the impression link today’s medical decision-making to those complications?
- Do your providers consistently document the link between a patient’s cancer and his or her presenting symptoms when it is clinically relevant?
Your Database Must Accurately Reflect Your Patients
ICD-10-CM has been in place long enough to begin evaluating the clinical demographic picture of your practice to ensure that you are well-positioned for the new reimbursement models.
Begin by running a frequency report of the diagnosis codes reported by your providers during the past 6 months. Query your providers, and determine the conditions they manage, or those that impact the care of their patients.
Consider the basics, such as how many patients are obese, insulin-dependent diabetics, or struggle with circulatory or respiratory disorders in addition to the hematology/oncology conditions that brought the patient to your practice; then simply compare that information with the reported codes. The message is clear that these patients’ diseases are complex, and it takes additional time, resources, and social services to manage their medical and socioeconomic struggles, but the data do not consistently support that message.
The concept of placing a different value on patients with severe complications or comorbidities is already being used in facility reimbursement. The challenge will be to ensure that the database used to design a similar process for physicians also accurately reflects the patients who are being treated.
If you want to be appropriately reimbursed under the new models in 2018, today’s database needs to accurately reflect the number of your patients whose complications or comorbidities impact their care by your providers.
References
- Goldstein A. Federal health officials, insurers agree on how to rate doctors’ quality. Washington Post. February 16, 2016. www.washingtonpost.com/national/health-science/federal-health-officials-insurers-agree-on-how-to-rate-doctors-quality/2016/02/16/e87934b0-d4d4-11e5-9823-02b905009f99_story.html. Accessed March 31, 2016.
- Mamula KB. Highmark unveils new cancer reimbursement plan to save patients money. Pittsburgh Post-Gazette. March 17, 2016. www.post-gazette.com/business/healthcare-business/2016/03/17/Highmark-has-new-reimbursement-plan-for-cancer-treatment/stories/201603170042. Accessed March 31, 2016.