On October 1, 2014, the United States will adopt the International Classification of Diseases, Tenth Revision, Clinical Modification/Procedure Coding System (ICD-10-CM/PCS). The reprieve, although welcome to many, is less than 16 months away, during which several phases of implementation must be completed. The timeline for implementing the code sets is divided into 4 phases: Phase 1: Impact Assessment, first quarter 2009 through second quarter 2012; Phase 2: Preparing for Implementation, first quarter 2012 through second quarter 2014; Phase 3: Go Live Preparation, first quarter 2013 through third quarter 2014; and Phase 4: Postimplementation, fourth quarter 2014 through fourth quarter 2015.
Phase 1: Impact Assessment
Your practice should already have completed the impact assessment. If you are behind schedule, you need to work hard now to catch up. The shift from International Classification of Diseases, Ninth Revision (ICD-9) involves serious challenges, including transitioning from a system of 13,000 codes to a system of more than 68,000 codes in ICD-10-CM.
You may recall that the implementation of a new generation of the 9 electronic standards for the Health Insurance Portability and Accountability Act (HIPAA), known as the American National Standards Institute (ANSI) Version 5010 (v5010), is a part of this process. ANSI v5010 replaced the electronic transaction standards ANSI v4010/v4010A. Once ICD-10-CM goes into effect, any transactions that are not compliant with HIPAA (ie, not using ANSI v5010) will be rejected. The new codes will be structurally different from the ICD-9 codes (Table 1 and Table 2). By now, you should have a steering committee in place or have devised a communication schedule involving everyone in your practice who will play a role in implementing the new coding system. If you have not already done so, you should take the following steps as soon as possible:
- Begin operational processes
- Evaluate workflow (data and staff)
- Identify how to improve workflow
- Conduct a gap analysis
- Modify your software and upgrade your hardware
- Educate your staff
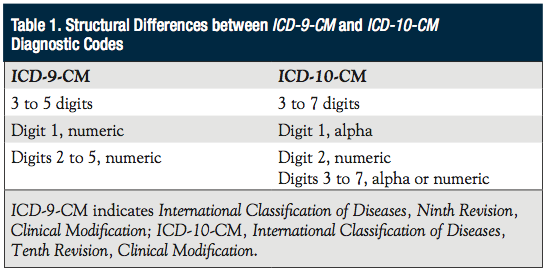
Table 1
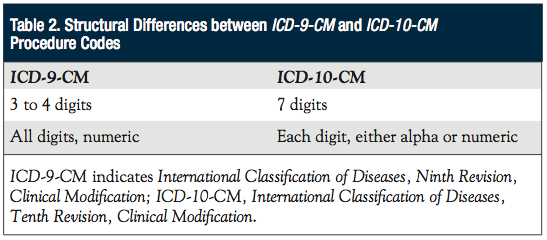
Table 2
Phase 2: Preparing for Implementation
Now is also the time for the staff to review the practice’s current procedures and improve upon them, making them more efficient and cost-effective. The newly provided codes were designed to ensure that the collected data reflect patients’ conditions more precisely, decrease claims rejections, and improve the benchmarking of data and public health records. Examine the systems, vendor contracts, and costs for both your electronic health records (EHRs) and practice management systems. Use the following questions as a guide through this process.
Are your contracts with payers ready for the move? You may need to review and update these contracts to pave the way for the move to ICD-10.
Will your current practice management system accommodate the change, or will you require a new system? Choose a software package that will accommodate the necessary changes. Review the problems your practice has experienced in the past 2 years and how they affected your practice and cash flow. Ask yourself what responses and issues you faced with your current practice management software vendor/customer support. How difficult was it to resolve any problems? What did it cost you in time, lost productivity, staffing, and overtime to “catch up” from having your system down for maintenance and upgrades?
Will the upgrade to the new system involve a fee? If so, how much will that cost? Will your vendor(s)provide the codes at no cost?
What is your vendor(s’) timeline for implementation, and when will they allow you to test your system? You will need to know when the upgrade to your existing system will be complete or when the entirely new system will be available. When it is complete, you then need to know whether your vendor(s) will provide training for your practice, and if so, what the training will cost.
Have you begun to modify your templates? Remember to update your forms and superbills. The newer forms will, by necessity, be far more comprehensive and complex than the older forms.
Will your vendor(s) load your specialty specifically, or will all of the specialties be included in your system? Will diagnoses be searchable by partial terms, and will they include the coding guidelines, rules, and exceptions to the guidelines that your practice may encounter? For example, when coding for malignancies, the malignancy will remain the principal diagnosis when the treatment is directed at the malignancy. However, if a patient is admitted for anemia associated with the malignancy and the treatment is exclusively for anemia, the code for the malignancy will be listed as the principal or first-listed diagnosis, followed by the code D63.0, Anemia in neoplastic disease.
Next Steps:
- Contract with a consulting service
- Redesign and reprint paper forms
- Convert your data
- Maintain a dual system until all of the problems with the new system have been worked out
- Purchase software, seek educational resources, and use mapping tools as needed to help with the transition
- Anticipate decreased coding accuracy and work to solve those associated issues
- Monitor coding from the point of implementation
- Develop a communications plan in preparation for going live
- Regularly update your senior executives
Phase 3: Go Live Preparation
Before you “go live,” be sure that any systems that are not working properly are corrected. Again, make sure you know what your vendor(s) will be able to do to help you with the transition. If you do not know for sure, ask your vendor(s) whether a mapping program will be provided. General Equivalence Mappings (GEMs) were developed to help you with the conversion, because ICD-10 is more specific than ICD-9.1
GEMs are basically translation tools for not only payers and providers, but anyone working with coded data. Remember, the diagnostic codes have increased from 14,025 to 68,069. Procedural codes have increased from 3824 to 72,589. The GEMs can be used to convert your data from ICD-9 to ICD-10-CM/PCS and back again (ie, forward and backward mappings, also known as crosswalks).
The GEMs will allow you to translate data for tracking quality, recording morbidity and mortality, calculating reimbursement, or converting an ICD-9-CM–based application to ICD-10-CM/PCS. They also can be used to help your practice convert payment systems, payment and coverage edits, risk adjustment logic, quality measures, and research applications germane to trend data. In cases where there is no translation between an ICD-9-CM code and an ICD-10 code, a flag will indicate “No Map.” One such example is ICD-9-CM Procedure Code 89.8—Autopsy, for which there is no translation in ICD-10-CM/PCS.
Next Steps:
- Confirm with your vendor(s) that the needed upgrades are in place
- Finalize all system changes from January through September 2014
- Complete testing
- Conduct claims testing
- Make any necessary modifications and reassign testing
- Have a contingency plan in place
Phase 4: Postimplementation
Reeducate your staff as necessary and continue to monitor all of your systems—cash flow, productivity, revenue, and coding accuracy.
Exceptions to the Rule
As one would expect, there are several exceptions to the rule. One occurs in the etiology/manifestation convention regarding placement of the code, as well as the placement of the notes “use additional code” and “diseases classified elsewhere.” Certain conditions have both an underlying etiology and multiple body system manifestations owing to the underlying etiology. For such conditions, the ICD-9 coding convention requires that the underlying condition be sequenced first, followed by the systemic manifestation(s). Wherever such a combination exists, there is a “use additional code” note at the etiology code, and a “code first” note at the manifestation code. These instructional notes indicate the proper sequencing order of the codes—etiology followed by manifestation.2
Another exception to the rule occurs with regard to syndromes. When coding syndromes, it is important to follow the alphabetical index guidance. When there is no index guidance, assign codes for the documented manifestations of the syndrome.2
Looking at the positive side of the ICD-10-CM/PCS transition, once we are prepared, trained, and on our way, the higher level of specificity with which this coding system will allow us to code will paint a very clear picture for the insurance carriers and will clearly identify patients’ medical problems to justify the medical services performed. All of this assumes, of course, that the provider is well educated on this system and is utilizing it to its fullest potential. The level of detail required should result in decreased requests from insurance carriers for medical records which, in turn, will allow the staff to work on other tasks that are critical to the daily operations of your medical practice.
Next Steps:
- Monitor the impact of ICD-10 on reimbursement
- Meet with your staff regularly to share information
- Monitor the functionality of your practice management and EHRs systems
- Monitor coding accuracy and productivity
- Train or retrain your staff as required
- Monitor your case mix
- Resolve payment issues
- Communicate with payers
Conclusion
A significant amount of concern and resistance remains in accepting ICD-10-CM/PCS. However, it is coming, and time is ticking away. It is better to take a look at things now, to take the first step and have the first meeting to see who in your organization knows anything about ICD-10-CM/PCS. Your first step may be to send someone to a seminar or assign someone to spend the time to research the basics online.
To fully participate in this system, it is highly recommended that you fully understand the coding guidelines. Although some of the guidelines have been retained, there are exceptions—particularly with the new combination codes.
It is important to remember that the ICD-10-CM codes will be used by all medical providers. The ICD-10-CM/PCS codes are only for inpatient hospital procedures and are used only by the hospitals. You must provide a full description of a procedure or diagnosis. It would be a grave error to truncate these codes, as we are attempting to seek the highest level of specificity. If your vendors download only partial codes, the data will not serve its purpose.1
References
1. General Equivalence Mappings. www.cms.gov/Medicare/Coding/ICD10/downloads/GEMS-Cross walksBasicFAQ.pdf. Accessed April 17, 2013.
2. American Medical Association. CPT® 2013 Professional Edition. 2013; American Medical Association. Last modified May 2, 2013.